
The last 5 years has seen a dramatic evolution in treatments for multiple myeloma. Previously, bortezemib, lenalidomide and pomalidamide, in combination with steroids and used sequentially, was the mainstay of treatment for transplant ineligible patients. With the introduction of carfilzomib, panobinostat, elotuzumab, daratumumab and ixazomib as add-ons to existing therapies, there is now a much large number of possible combinations and sequences.
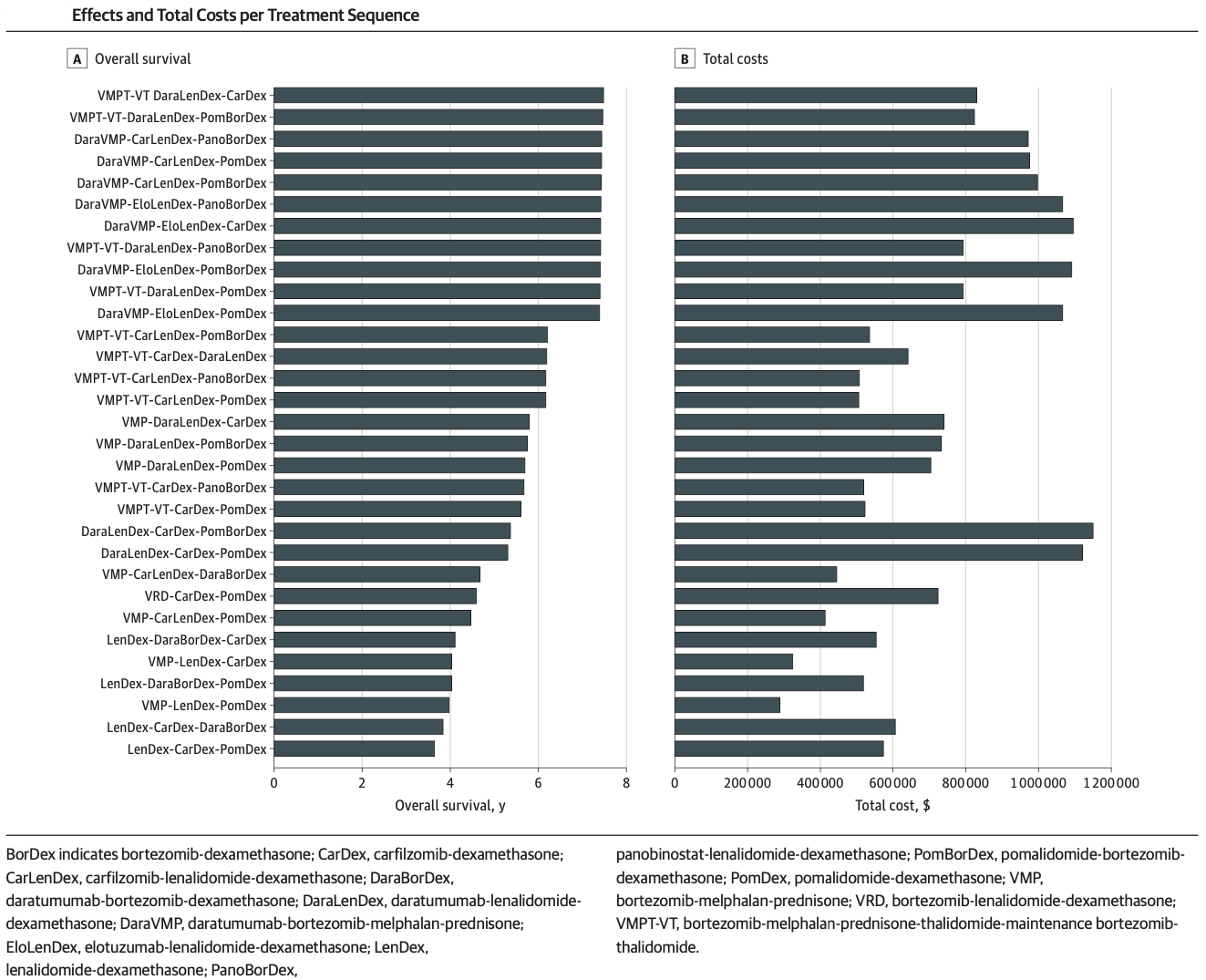
Pivotal clinical trials in early therapy lines focus on PFS endpoints. However, the best PFS results in early lines may not translate to best OS results, if the early line regimen uses up the most efficacious treatments for subsequent lines. Different sequences can also have very large differences in costs, without significant difference in OS.
Blommestein et al illustrate this in a modelling study that attempts to compare outcomes, costs and cost-effectiveness of a wide range of possible treatment sequences. Their approach has important limitations, but provides valuable insights and is a useful complement to the incremental approach to assessing new myeloma treatments that is typically applied in HTA.
https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2777838






